What if detecting the most lethal form of brain cancer required nothing more than one microliter of cerebrospinal fluid — less than a teardrop — and could deliver results with zero false negatives? A team at Peking University Third Hospital has turned this possibility into reality with a biosensor so sensitive it operates at the zeptomolar scale — detecting molecular concentrations 10²¹ times more dilute than a mole per liter.
The study, led by neurosurgeon Jun Yang (杨军) and published in Advanced Science (IF 14.1, CAS Zone 1) on April 27, 2026, represents a potential paradigm shift in how brain tumors are diagnosed and monitored — moving from invasive brain biopsies toward a simple, rapid liquid biopsy.
The Glioma Diagnosis Challenge: Why We Need Better Tools
Gliomas are the most common primary brain tumors in adults, ranging from slow-growing lower-grade tumors to the devastating glioblastoma, which has a median survival of just 15 months. Diagnosing a glioma and determining its molecular subtype — critical for treatment decisions — currently requires an invasive brain biopsy or surgical resection.
The challenges are significant:
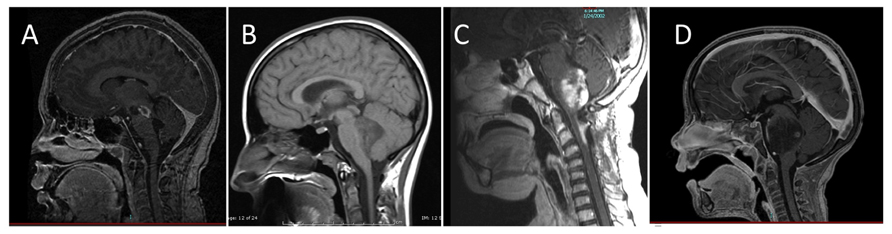
- MRI cannot determine molecular subtype. Imaging shows the tumor’s location and size but cannot reveal the IDH mutation status, MGMT methylation, or other molecular features that guide therapy.
- Stereotactic biopsy is invasive and risky. Needle biopsy carries risks of hemorrhage (1-3%), infection, and neurological deficit. Critically, it samples only a tiny portion of the tumor, potentially missing the most aggressive regions due to tumor heterogeneity.
- Biopsies cannot be repeated easily. Tumors evolve over time and in response to treatment. Monitoring molecular changes requires repeated sampling — something that is impractical with invasive biopsies.
- Symptoms are often nonspecific. Headaches, nausea, and cognitive changes can be attributed to many conditions, delaying diagnosis until the tumor is advanced.
Circulating Tumor DNA and the Blood-Brain Barrier Problem
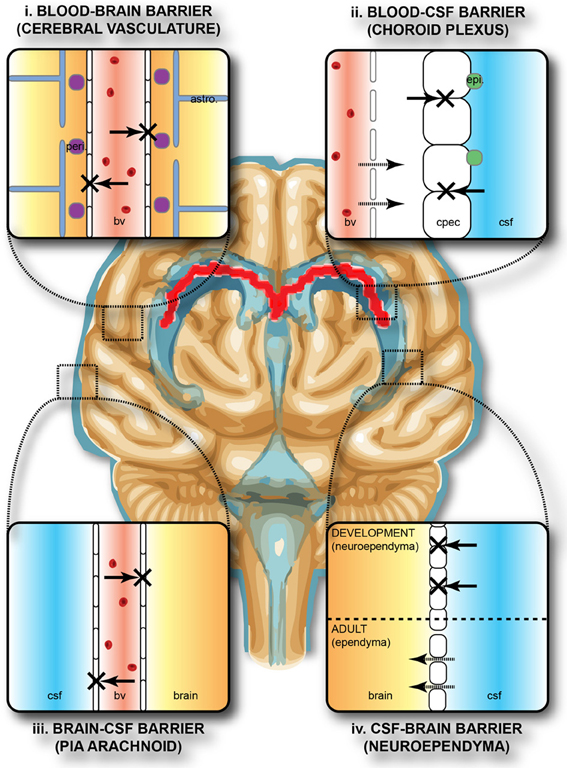
Liquid biopsy — detecting tumor-specific DNA fragments in body fluids — has transformed cancer diagnostics for many solid tumors. In brain tumors, however, the blood-brain barrier (BBB) severely limits the amount of circulating tumor DNA (ctDNA) that reaches the bloodstream. ctDNA concentrations in the blood of glioma patients are often too low to detect with conventional methods.
Cerebrospinal fluid (CSF), which bathes the brain and spinal cord directly, is a far richer source of glioma ctDNA. CSF is in direct contact with the tumor microenvironment, and ctDNA concentrations in CSF are significantly higher than in plasma. However, even in CSF, ctDNA from brain tumors exists at extremely low concentrations — often in the femtomolar to attomolar range — challenging the limits of existing detection technologies.
Current methods like droplet digital PCR (ddPCR) and next-generation sequencing (NGS) have sensitivity limits typically in the femtomolar to picomolar range, require relatively large sample volumes (10-100+ microliters), and can yield false negatives when ctDNA abundance is very low.
The Breakthrough: A Dual-Channel Zeptomolar Biosensor
The PKU Third Hospital team, in collaboration with the National Innovation Institute of Defense Technology, developed what they call the Dual-Channel Synergistic Ultrasensitive Biosensor (DCSU-Biosensor). The platform combines two powerful technologies: a quantum-bound states in the continuum (Q-BIC) metasurface and a DNA nanotechnology cascade amplification system.
The result: a detection limit of 74 zM (zeptomolar) — that is 74 × 10⁻²¹ moles per liter, or roughly 45 target molecules in a microliter sample. This is 6-9 orders of magnitude more sensitive than conventional ddPCR.
The study was published in Advanced Science on April 27, 2026 (DOI: 10.1002/advs.75443), with co-corresponding authors Jun Yang (PKU Third Hospital Neurosurgery), Qinggang Ge (PKU Third Hospital ICU), and Chao Chang (National Innovation Institute of Defense Technology).
How It Works: Metasurface Meets DNA Nanotechnology
The DCSU-Biosensor operates through a two-stage signal enhancement strategy:
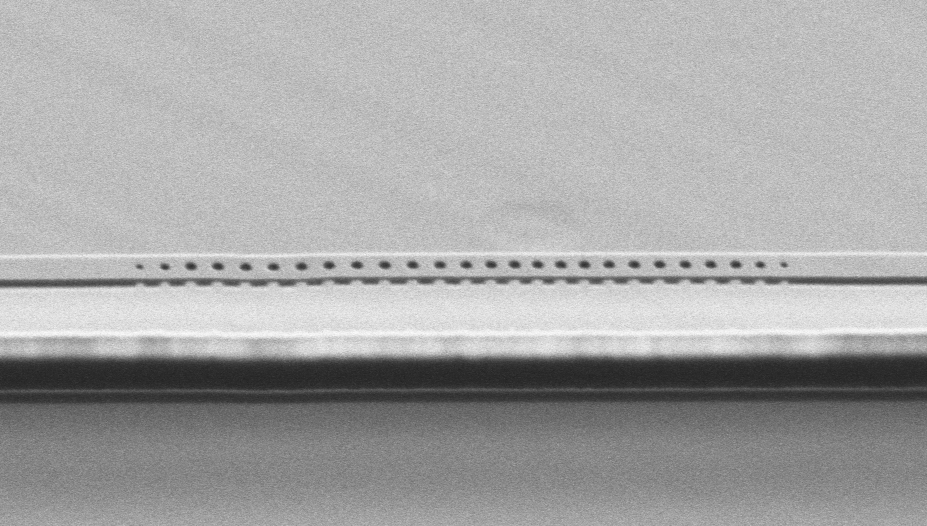
Stage 1: Q-BIC Metasurface — Optical Enhancement
The metasurface uses carefully engineered nanostructures that support quasi-bound states in the continuum (Q-BIC) — a photonic phenomenon that dramatically concentrates electromagnetic energy at the sensing interface. By introducing structural symmetry breaking and momentum condition regulation, the researchers achieved a quality (Q) factor of 197, overcoming the inherent field confinement limitations of conventional metasurfaces.
Stage 2: DNA Tetrahedron-HCR-AuNP Cascade — Biochemical Amplification
On top of the optical enhancement, a three-component biochemical amplification system further boosts the signal:
- DNA tetrahedron (TDN) — a rigid, 3D DNA nanostructure that positions the capture probe with precise spatial orientation
- Hybridization chain reaction (HCR) — an enzyme-free, isothermal DNA amplification generating long double-stranded DNA polymers
- Gold nanoparticles (AuNP) — attached to HCR products, providing massive refractive index changes at the metasurface surface
When the target IDH1.R132H ctDNA binds to the capture probe, it triggers the entire cascade, producing a dual-channel optical signal change detectable at zeptomolar concentrations.
Performance That Shatters Existing Limits
| Metric | DCSU-Biosensor | Droplet Digital PCR |
|---|---|---|
| Detection Limit | 74 zM (10⁻²¹ M) | ~fM-pM (10⁻¹⁵ to 10⁻¹² M) |
| Dynamic Range | 12 orders of magnitude | 3-4 orders of magnitude |
| Sample Volume | 1 µL | 10-100+ µL |
| Clinical Sensitivity | 93.33% | Lower at low ctDNA |
| False Negatives | 0 | Higher at low ctDNA |
| Label-Free | Yes | No (requires probes) |
| Cost | Low | Moderate-High |
The biosensor can distinguish the IDH1.R132H mutation from IDH1 wildtype and other R132 mutation subtypes — essential for clinical decision-making in glioma subtyping per WHO 2021 classification.
Clinical Validation: 93.33% Sensitivity, Zero False Negatives

The researchers validated the biosensor using 40 clinical CSF samples from three groups: healthy controls, IDH1-wildtype glioma patients, and IDH1.R132H-mutant glioma patients. The results were striking:
- Clinical sensitivity: 93.33% — correctly identifying the vast majority of IDH1.R132H-mutant tumors
- Zero false negatives — no mutant tumors were missed, a critical metric for diagnostic tests
- CSF outperformed plasma — CSF samples showed significantly stronger detection responses
- Detection signal correlated with tumor volume and glioma grade — suggesting potential for quantitative tumor burden monitoring
This means the biosensor could potentially be used not just for initial diagnosis, but for monitoring treatment response and detecting recurrence — all from a minimally invasive lumbar puncture rather than repeat brain surgery.
What This Means for Patients and the Future of Brain Tumor Care

The implications of this technology extend well beyond a single detection platform:
For diagnosis: Patients with suspected glioma could receive molecular subtyping through a lumbar puncture rather than an invasive brain biopsy. This is especially valuable for tumors in eloquent brain areas where biopsy carries high neurological risk.
For monitoring: After initial treatment, patients could undergo periodic CSF testing to detect molecular recurrence before it becomes visible on MRI — potentially enabling earlier intervention.
For research: The ability to detect ctDNA at zeptomolar concentrations opens new avenues for understanding tumor biology, heterogeneity, and evolution at unprecedented resolution.
For accessibility: The label-free, rapid, and low-cost nature of the platform could eventually make high-sensitivity glioma screening available in resource-limited settings.
Why This Matters for International Patients
For international patients seeking brain tumor diagnosis or second opinions in China, this technology represents a significant advance. PKU Third Hospital’s Neurosurgery Department, led by Jun Yang, is one of China’s premier neurosurgical centers, and the integration of this biosensor into clinical workflow could offer patients a less invasive, faster, and more sensitive diagnostic pathway.
The ability to obtain molecular tumor information from just 1 microliter of CSF — with zero false negatives — means that even small-volume lumbar puncture samples can yield definitive results, reducing the need for repeated invasive procedures and accelerating the path to personalized treatment.
Sources
- Sun Y, Zhang J, Liu C, et al. A Dual-Channel Synergistic Ultrasensitive Biosensor for Tumor Liquid Biopsy. Advanced Science. 2026. DOI: 10.1002/advs.75443 | PubMed: 42043839
- PKU Medical News: “北京大学第三医院杨军团队发表成果:发现脑脊液检测胶质瘤的超灵敏新方法” (June 12, 2026)
- BrainMed “中国声音” Column: “ADV SCI|以微升级脑脊液实现胶质瘤IDH1突变精准检测” (June 5, 2026)
- Pérez-Alfayate R, et al. Cerebrospinal fluid ctDNA as a diagnostic and prognostic tool in gliomas: systematic review and meta-analysis. Front Oncol. 2025;15:1714287.