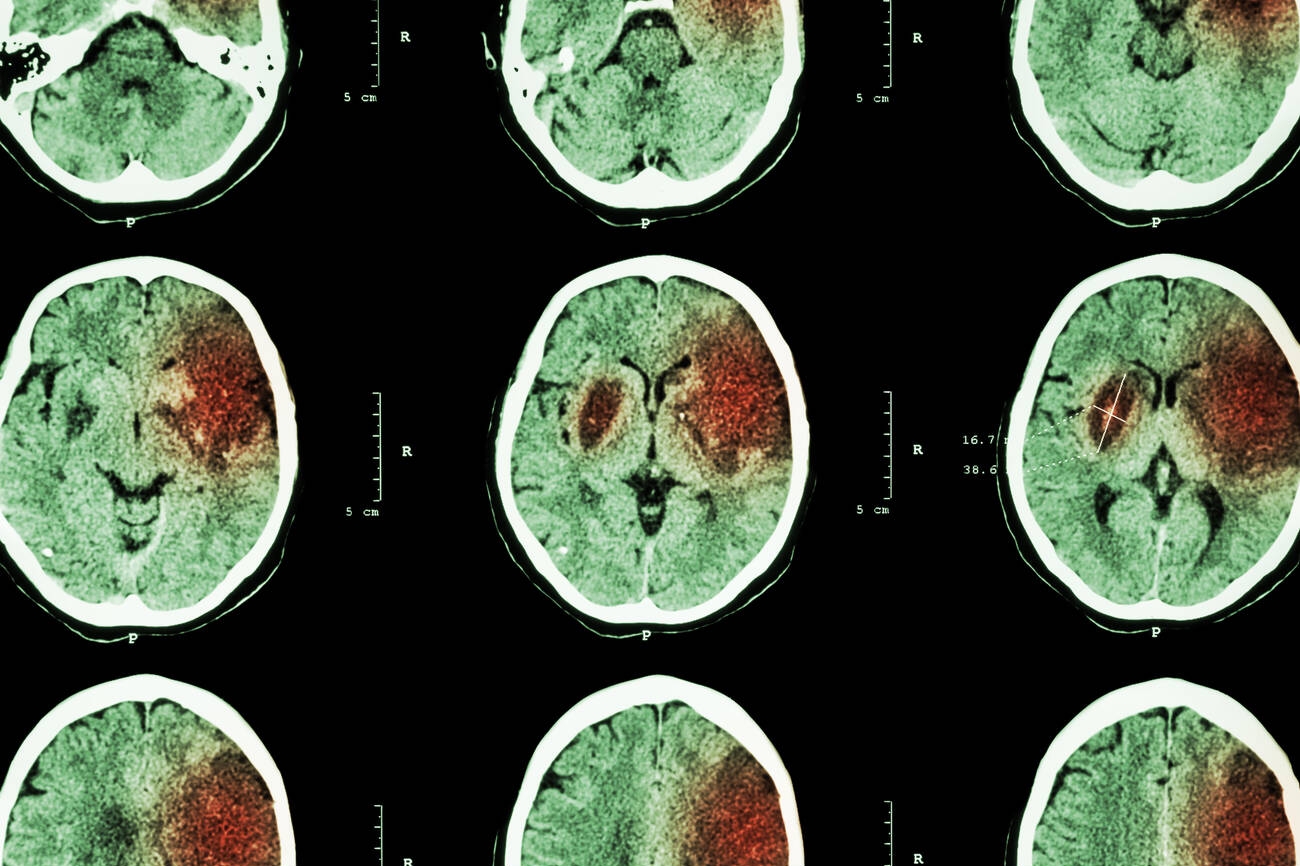
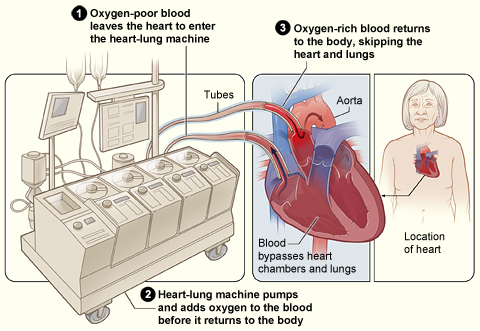
Imagine this: a patient lies in the ICU with a heart valve destroyed by infection. Septic emboli have already lodged in their brain, causing a stroke. The infected valve must be replaced — but open-heart surgery requires blood thinners and a heart-lung bypass machine, either of which could turn a small brain bleed into a catastrophic hemorrhage. Delay the surgery, and the infection may throw more clots to the brain, worsen heart failure, or kill the patient outright.
This is the “heart-brain dilemma” — one of the most agonizing decisions in cardiac surgery. For decades, doctors had little evidence to guide them. Now, a landmark study from Peking Union Medical College Hospital (PUMCH), published in the Journal of the American Heart Association (JAHA), provides the first comprehensive, evidence-based framework for resolving it.
What Is Infective Endocarditis — And Why Does It Attack the Brain?
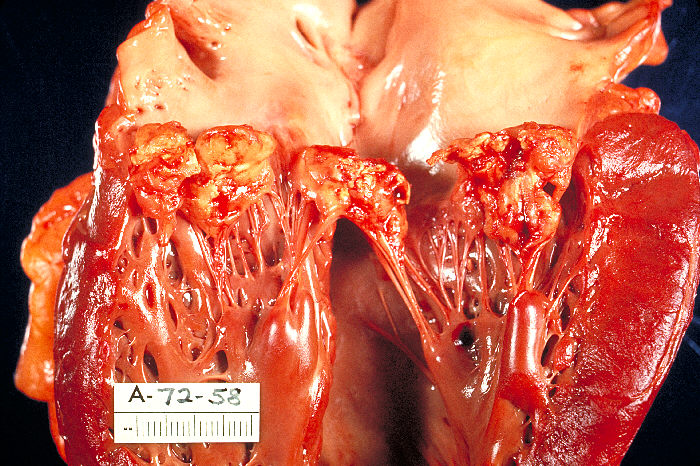
Infective endocarditis (IE) is a life-threatening infection of the heart’s inner lining and valves, typically caused by bacteria entering the bloodstream. The infection creates vegetations — clumps of bacteria, blood cells, and fibrin — on valve surfaces. These vegetations are fragile; pieces break off and travel through the bloodstream as septic emboli.
The brain is among the most vulnerable targets. Between 20% and 40% of IE patients develop neurological complications, including ischemic stroke, hemorrhagic transformation, intracerebral hemorrhage, infectious intracranial aneurysms, and subarachnoid hemorrhage. Mortality in these patients can reach 45% — nearly half die.
Common causative organisms include Staphylococcus aureus, viridans group streptococci, and enterococci. Risk factors include prosthetic heart valves, congenital heart disease, intravenous drug use, and indwelling catheters.
The Heart-Brain Dilemma: Operate Now or Wait?
The clinical dilemma is brutally simple:
Operate early, risk the brain. Cardiac surgery requires systemic heparinization (blood thinning) and cardiopulmonary bypass, which can convert an ischemic stroke into a hemorrhagic one, enlarge an existing brain bleed, or trigger new intracranial hemorrhage.
Delay surgery, risk the heart. Without surgery, the infected valve continues shedding septic emboli — causing more strokes. Heart failure worsens. The infection spreads. The patient may die of sepsis or cardiogenic shock before surgery ever happens.
Current international guidelines — the 2023 European Society of Cardiology (ESC) recommendations — advise postponing cardiac surgery for approximately four weeks after an ischemic stroke and even longer after intracranial hemorrhage. However, these recommendations are based on low-quality evidence (Class IIa/IIb, Level B/C) and do not differentiate by hemorrhagic transformation subtype or neurological severity.
No randomized controlled trial has ever addressed this question. Doctors have been making life-or-death decisions based on expert opinion and small case series.
The PUMCH Study: 663 Patients, 12 Years, One Answer

The PUMCH team, led by cardiac surgeons Jun Zheng (郑军) and Chaoji Zhang (张超纪), conducted a retrospective cohort study spanning December 2012 to December 2024 — 12 years of consecutive surgical IE patients at China’s most prestigious hospital. The study enrolled 663 patients who underwent left-sided IE surgery; 204 (30.8%) had preoperative neurological complications.
Using propensity score matching and multivariable logistic/Cox regression, the researchers compared outcomes between patients with and without neurological complications, then drilled down into the relationship between specific neurological event types, surgical timing, and survival.
The study was published in JAHA on April 22, 2026 (online) with DOI 10.1161/JAHA.125.047207 and is freely accessible as an open-access article.
Surgical Timing: Not One-Size-Fits-All
The most clinically impactful finding is a nuanced, evidence-based surgical timing framework:
For ischemic stroke without hemorrhagic transformation: Do not delay surgery. Operating promptly does not increase mortality risk. Delayed surgery (beyond 30 days) was associated with worse outcomes, likely because the ongoing infection caused additional embolic events and cardiac deterioration.
For intracerebral hemorrhage (ICH): Early surgery (within 7 days of hemorrhage) is associated with significantly elevated mortality risk. Waiting approximately 14 days allows the risk to decline and stabilize, making surgery safer. However, excessive delay must be avoided to prevent cardiac deterioration.
This is a critical refinement of existing guidelines. The ESC 2023 guideline’s blanket “wait 4 weeks” recommendation may be too conservative for ischemic stroke without hemorrhage and insufficiently nuanced for ICH, where the risk trajectory is time-dependent rather than a simple threshold.
Valve Strategy: Biological Valves Reduce Bleeding Risk

The study also found that valve selection matters significantly in this high-risk population. Mitral valve repair and bioprosthetic valve implantation were associated with additional survival benefits compared to mechanical valves.
The reason: mechanical valves require lifelong anticoagulation with warfarin, which carries an ongoing risk of intracranial hemorrhage — a devastating complication in patients who have already suffered a brain bleed. Bioprosthetic valves require only short-term or no anticoagulation, effectively reducing the long-term risk of recurrent intracranial bleeding.
This finding aligns with a growing trend in the field, but PUMCH’s data provides the strongest evidence yet specifically for the IE-with-neurological-complications population.
Five-Level Risk Stratification: A New Clinical Roadmap

Beyond timing and valve selection, the PUMCH team constructed a five-level risk stratification system that integrates neurological event type and severity, providing a decision algorithm for clinicians. The system considers:
- Hemorrhagic transformation (HT) vs. parenchymal hematoma (PH) after cerebral infarction
- Infectious intracranial aneurysm (IIA) presence, location, and rupture status
- Subarachnoid hemorrhage (SAH)
- NIHSS score (National Institutes of Health Stroke Scale) for neurological severity
- Intracerebral hemorrhage (ICH) volume and location
Each risk level maps to a specific management pathway, from emergency surgery to delayed intervention with neurological monitoring. This transforms what was once an intuitive, experience-based decision into a structured, reproducible clinical algorithm.
Results That Speak for Themselves
Applying this framework at PUMCH, the mortality rate for IE patients with neurological complications was reduced to 8.8% — a dramatic improvement over the historical 45% mortality cited in the literature. Furthermore, over 80% of patients who had preoperative brain injury achieved good neurological recovery after surgery.
These results suggest that with appropriate risk stratification and timing, the vast majority of IE patients with brain complications can survive and regain neurological function — an outcome that would have been considered unlikely just a few years ago.
Independent risk factors identified in the study include peripheral vascular disease, mitral valve IE location, and S. aureus infection — information that can help clinicians identify the highest-risk patients preoperatively.
Why This Matters for International Patients

Infective endocarditis is a global disease. It affects patients worldwide regardless of geography, and the heart-brain dilemma is universal — no hospital anywhere has had high-quality evidence to guide these decisions.
PUMCH’s study, based on one of the largest surgical IE cohorts ever assembled, provides evidence that is immediately applicable worldwide. The five-level risk stratification system, the surgical timing recommendations, and the valve strategy insights give clinicians a concrete, evidence-based framework where none existed before.
For international patients considering cardiac surgery in China, PUMCH’s demonstrated expertise in managing this particularly complex complication — achieving 8.8% mortality where historical rates were 45% — represents a compelling reason to seek care at a center with this depth of experience.
Sources
- Yu R, Liang T, Wang X, et al. Neurological Complications and Surgical Outcomes in Infective Endocarditis. Journal of the American Heart Association. 2026;15(9):e047207. DOI: 10.1161/JAHA.125.047207 | PubMed: 42017329
- PUMCH Official News: “从’心脑两难’到’心脑同治’” (June 15, 2026). https://www.pumch.cn/detail/45721.html
- Delgado V, Ajmone Marsan N, et al. 2023 ESC Guidelines for the management of endocarditis. European Heart Journal. 2023;44(39):3948-4042. DOI: 10.1093/eurheartj/ehad193
- Musleh R, Schlattmann P, et al. Surgical Timing in IE with Intracranial Hemorrhage: Systematic Review and Meta-Analysis. JAHA. 2022. DOI: 10.1161/JAHA.121.024401
- Siquier-Padilla J, et al. Optimal Timing for Cardiac Surgery in IE with Neurological Complications. J Clin Med. 2022;11(18):5275.
- Bonaros N, et al. IE and neurologic events: indications and timing for surgical interventions. Eur Heart J Suppl. 2020;22(Supplement_M):M19.