Deep brain stimulation (DBS) has transformed the lives of millions of Parkinson’s disease patients worldwide. By implanting electrodes that deliver precise electrical pulses to specific brain regions, DBS can dramatically reduce tremors, rigidity, and the motor fluctuations that medication alone cannot control. Yet for all its clinical success, DBS has remained a treatment of the privileged — patients living near major medical centers with specialized programming expertise. Those in rural or remote areas face a stark choice: endure repeated expensive and exhausting long-distance travel, or forego optimal treatment entirely.
A landmark study published in Nature Health, drawing data from over 20,000 Parkinson’s disease patients across 439 Chinese hospitals, now demonstrates that remote programming for DBS devices delivers clinical outcomes matching in-person care while slashing healthcare inequality by 30% faster than conventional approaches. This finding carries profound implications for the 10 million Parkinson’s patients worldwide who struggle to access postoperative care.
The Geography of Inequality

World-class neurosurgical centers cluster in major cities like Beijing, Shanghai, and Guangzhou, while vast rural regions have little or no DBS programming capacity. The study quantified this burden starkly: a single programming visit costs patients in Xinjiang an average of 3,181 CNY, equivalent to 410% of annual per capita income, compared with roughly 800 CNY for patients in Beijing or Shanghai.
The consequence is a devastating feedback loop. Patients who cannot return for programming either endure suboptimal stimulation settings or abandon therapy entirely. This inequity characterizes DBS care not only in China but in every country with significant rural populations.
How Remote Programming Works
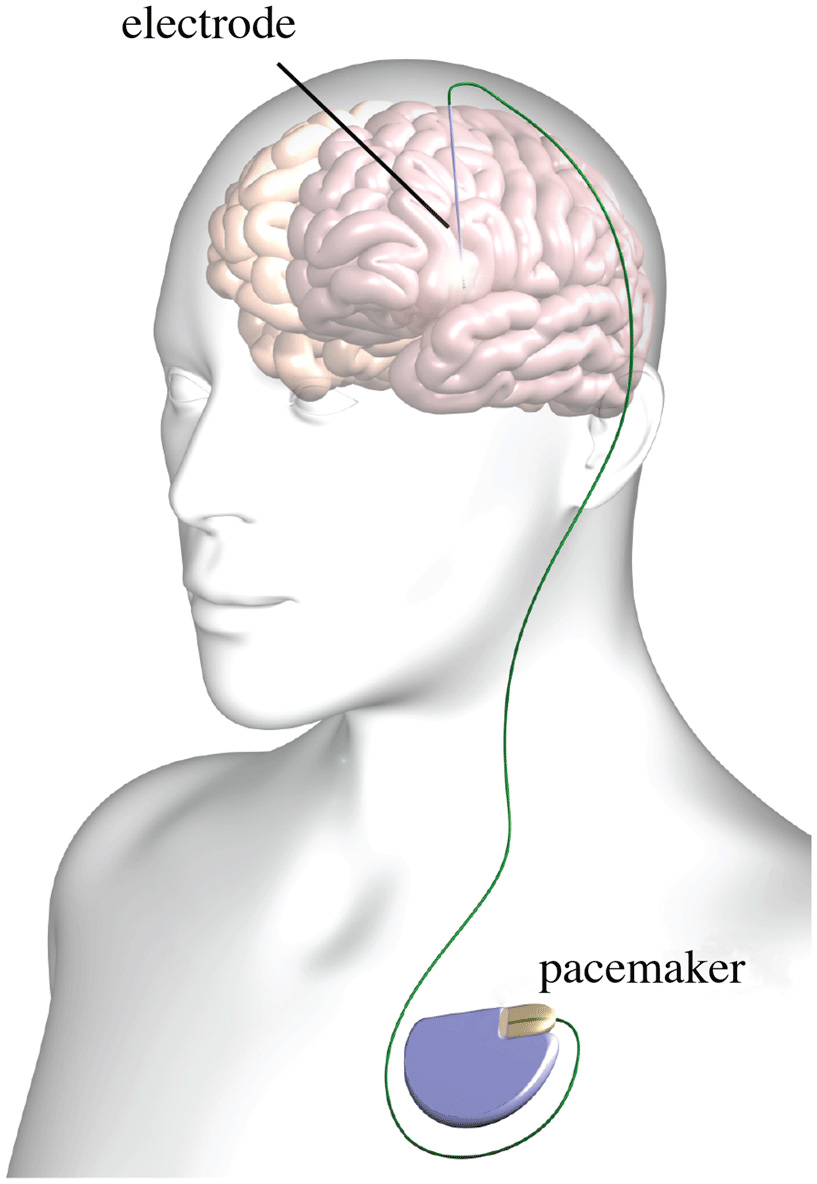
Remote programming exploits the wireless telemetry already built into modern neurostimulators. The patient sits at home or in a local clinic with a clinician programmer device placed over the implanted pulse generator. Through a secure internet connection, a specialist neurologist at a distant center conducts a structured motor examination via video and transmits new stimulation parameters directly to the implanted device.
The system incorporates two-factor authentication, real-time symptom recording, and a one-touch restoration feature that can instantly revert to the previous setting if needed. The platform, developed at Tsinghua University’s National Engineering Research Center for Neuromodulation (NERCN), has been refined through a decade of clinical iteration.
Clinical Results: Equivalence at a Distance
The central clinical question—does remote programming work as well as being there in person?—is answered with striking clarity. Among 3,048 patients across 216 centers, patient satisfaction scores on a 5-point scale were virtually identical: remote programming (RP) patients reported a mean satisfaction of 4.31, compared with 4.34 for onsite programming (OP) patients. The Patient Global Impression of Improvement showed no meaningful gap: RP scored 1.91 versus OP at 1.84.
Propensity score matching confirmed these results were not artifacts of patient selection. The study reports zero serious adverse events and zero device malfunctions attributable to remote programming. The one-touch restoration feature allows instant reversion to the last known good configuration.
A New Metric for Healthcare Equity

Perhaps most consequentially, the study introduces the Demographically Adjusted Parkinson Care Inequality Index (DPII). Before widespread RP adoption, the DPII for remote-accessible programming stood at 0.64 in 2017. By 2020, the RP DPII had fallen to 0.24, and by 2023-2024 it reached approximately 0.20—a 30% faster improvement than conventional expansion of in-person services.
This differential represents real patients who gained access to specialist DBS programming for the first time—not because a new hospital opened, but because the internet carried expertise to them.
Economic Projections for an Aging Population
The study’s economic modeling projects direct savings of 1.09 billion CNY per year through eliminated travel costs, with indirect savings through labor market participation reaching 8.15 billion CNY annually. By 2050, cumulative savings could reach 115 to 270 billion CNY.
China’s experience offers a replicable template. India, Brazil, and even the United States face similar urban-rural healthcare gradients. The technical requirements—reliable internet, telemetry-capable devices, and secure software—are increasingly available worldwide.
Remote Programming: A Global Model

For Parkinson’s patients worldwide, the implications are transformative. A technology that was once the privilege of urban residents near major medical centers can now reach the rural majority. The study’s 40+ investigators from 37 institutions have created not just a clinical validation but a methodological blueprint for telemedicine’s impact on equity.
The research team from Tsinghua University and Beijing Tsinghua Changgung Hospital, led by Professor Luming Li and including contributors from PLA General Hospital, has demonstrated that sophisticated neurological assessment and device adjustment can be performed over a network connection with the same outcomes as in-person care—while dramatically expanding access.
Sources:
- Lu Y, Sun Y, Guan D, Li L et al. “Remote programming for deep brain stimulation reduces healthcare inequality.” Nature Health, June 12, 2026.
- DOI: 10.1038/s44360-026-00131-z
- Zenodo Data Repository — Study Dataset and Supplementary Materials
- Tsinghua University — National Engineering Research Center for Neuromodulation (NERCN)